手术流程
本期医学手绘为UBE腰椎间盘摘除及同侧侧隐窝减压的手绘流程
info:
Lt. side case
L4/5 for example
左侧病例,以L4/5节段为例
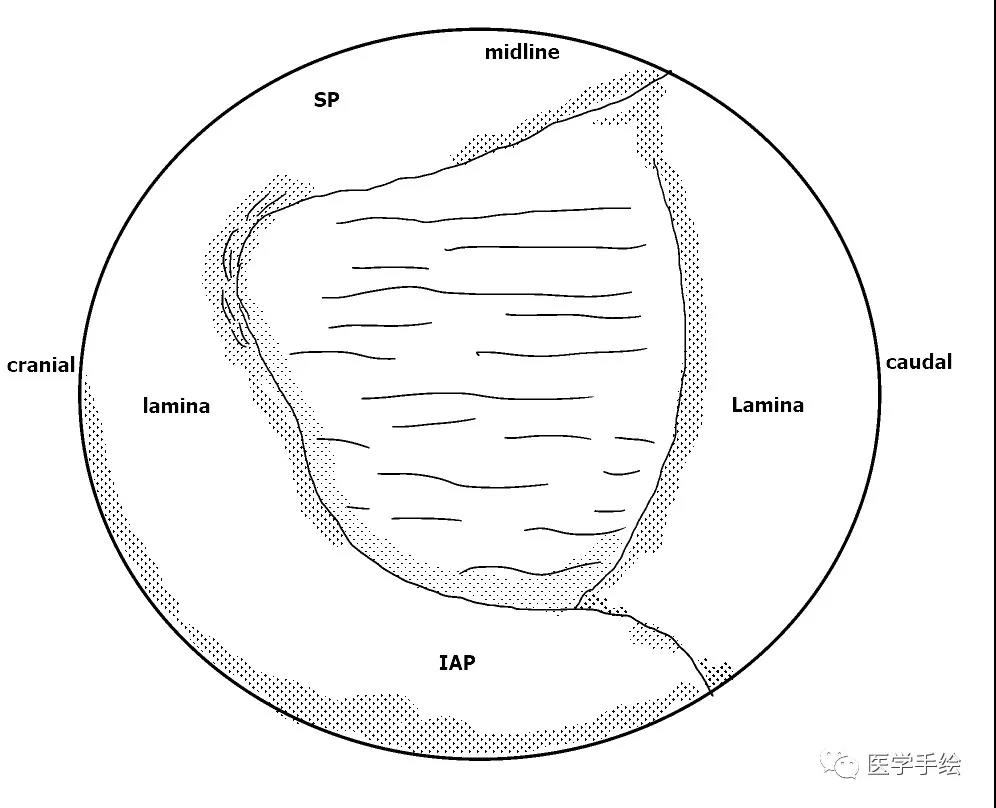
1. floor anatomy in Multifidus triangle area(建立通道后的多裂肌三角“地板解剖”)
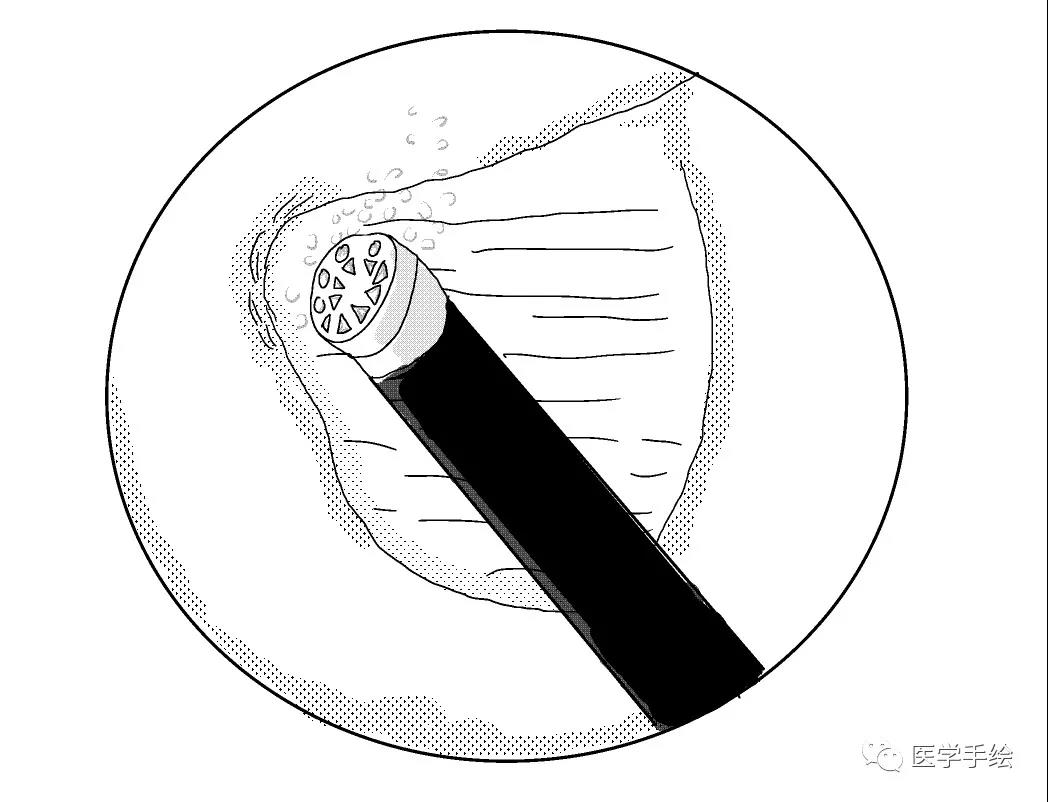
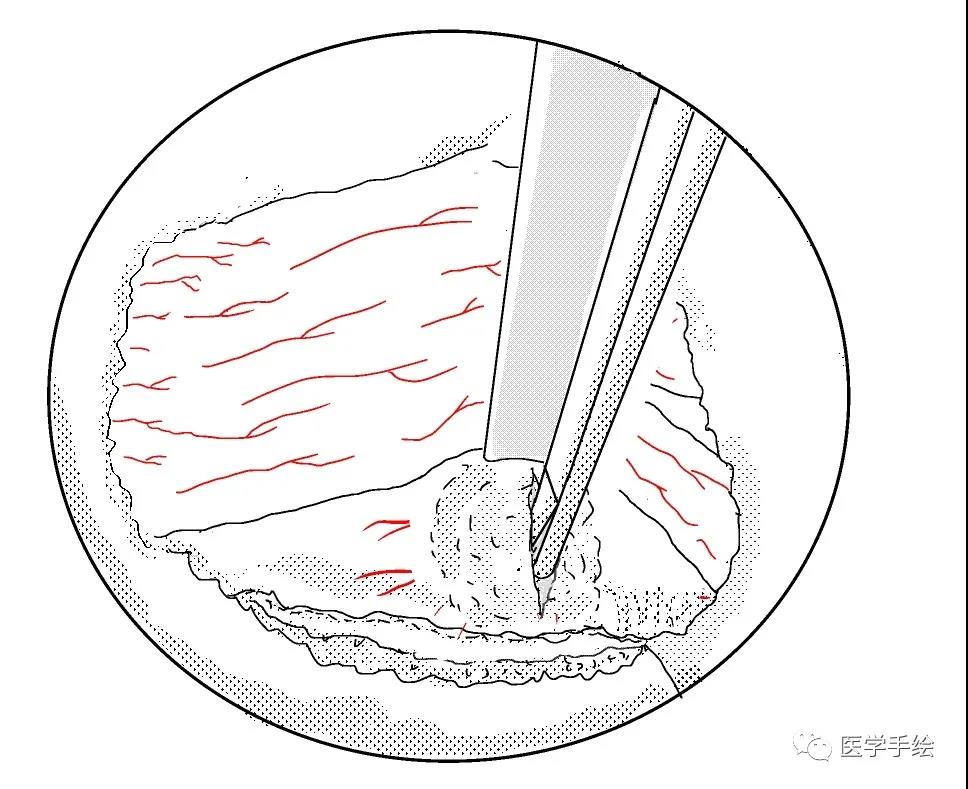
2. to clear the soft tissue on the surface of floor anatomy(大刀头清理软组织)
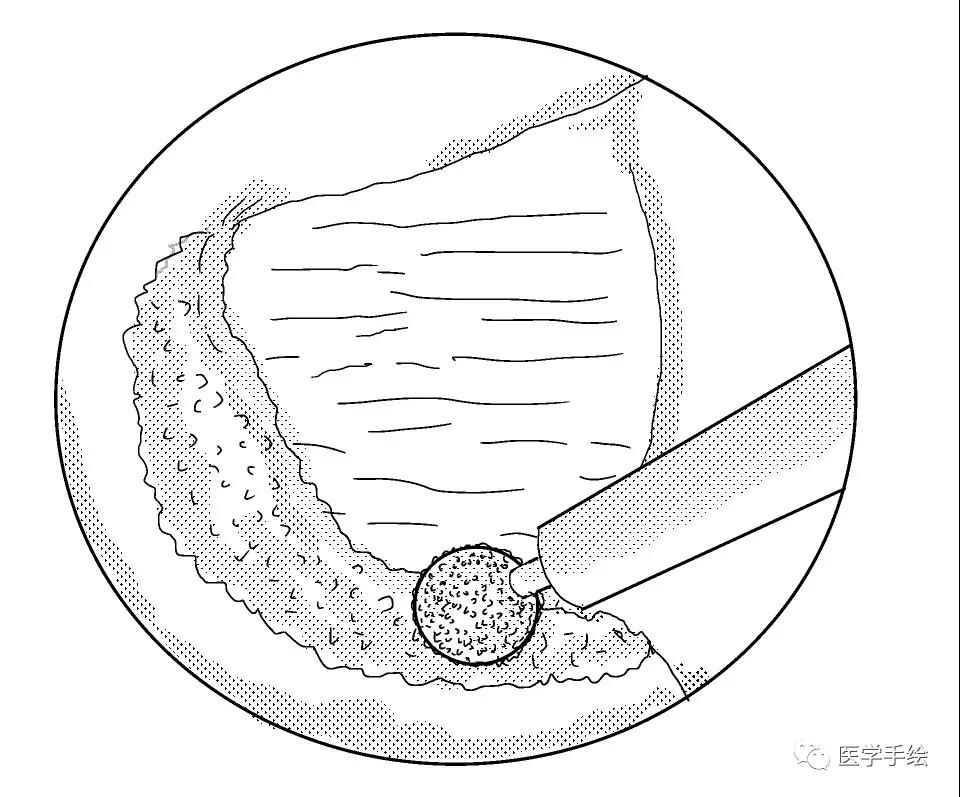
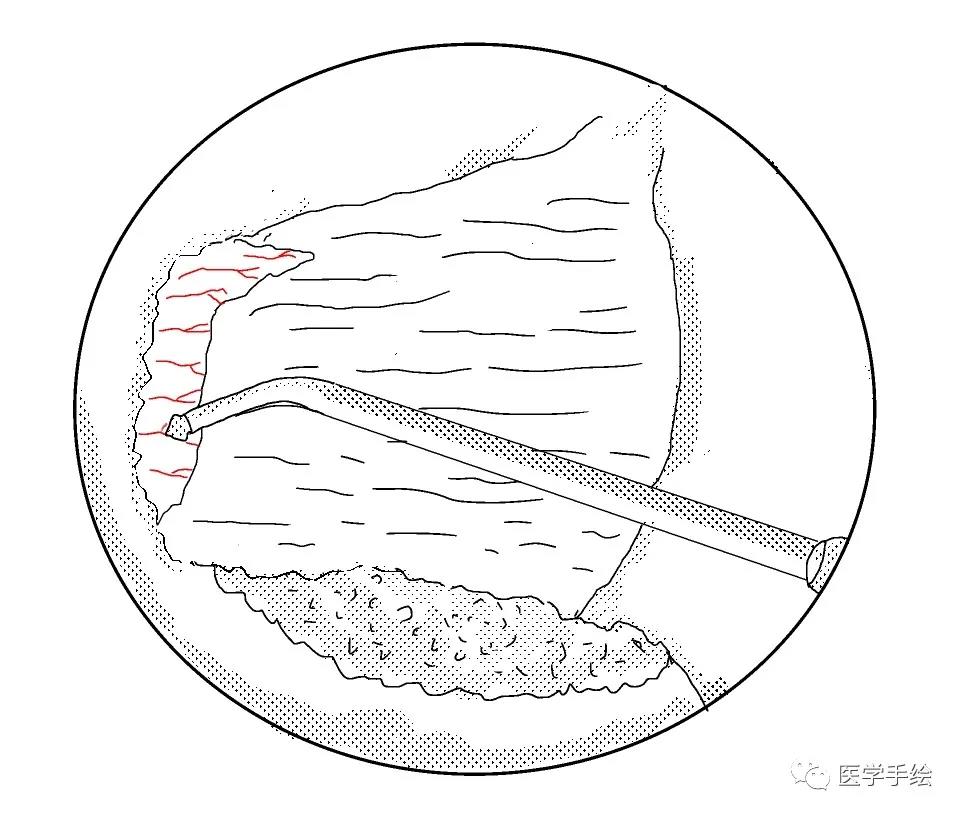
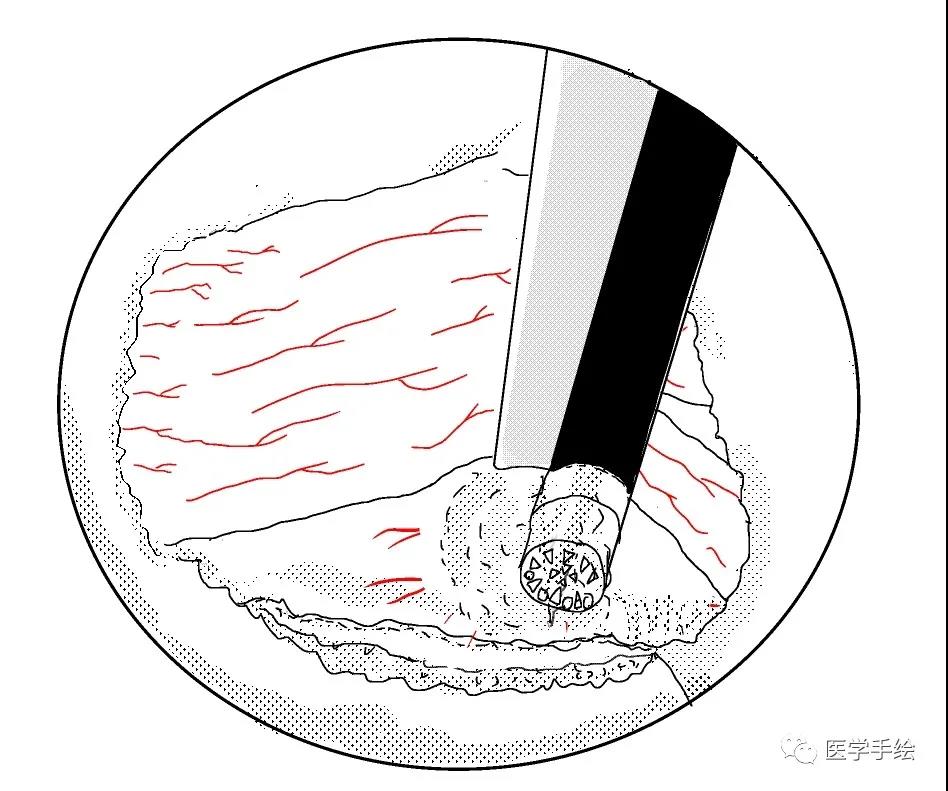
3. bonework by high speed diamond bur(使用4mm金刚砂磨钻将椎板下缘及下关节突内缘磨薄)
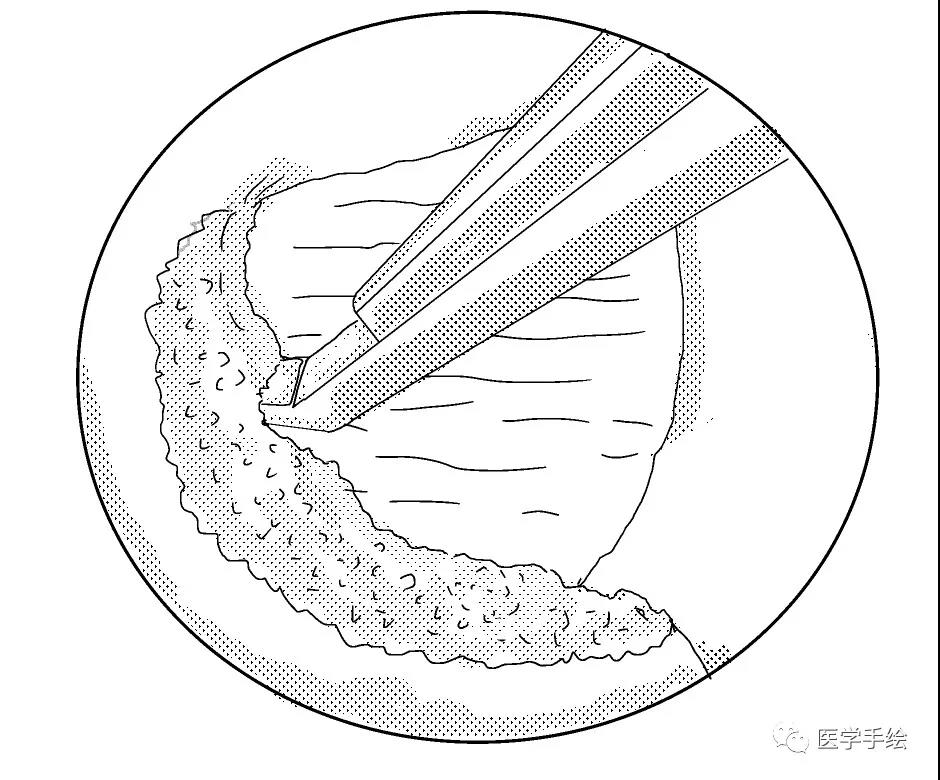
4. bonework by kerrison punch until you found the proximal insertion of FL(使用椎板咬骨钳继续向近端咬除椎板直至黄韧带近端止点)
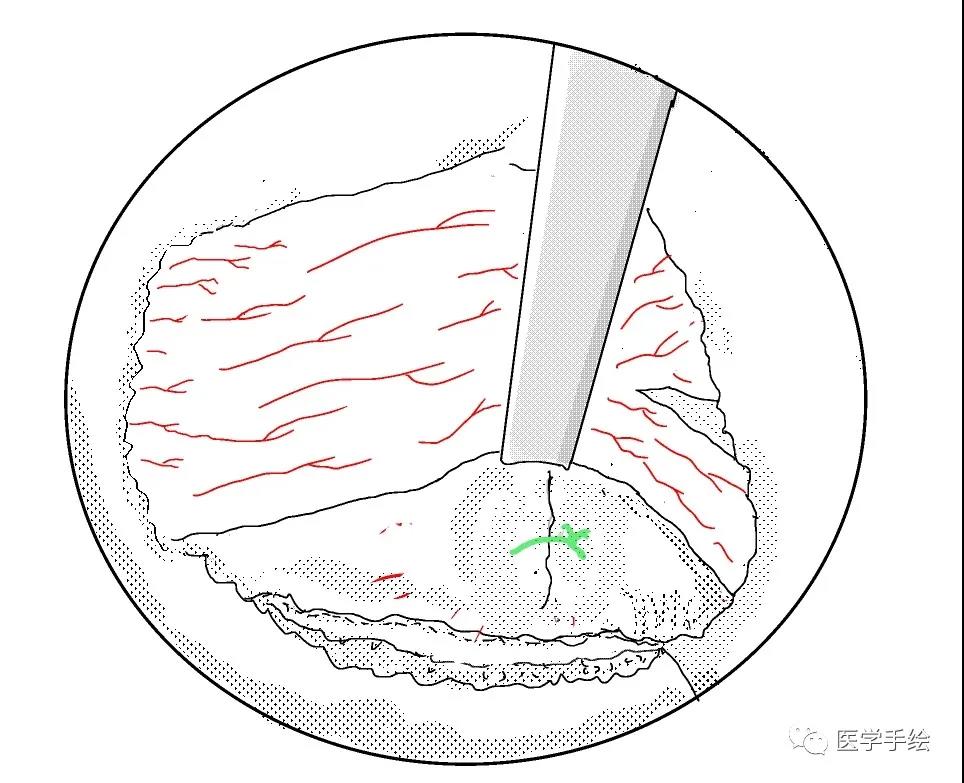
5. bleeding control by small size RF in proximal insertion of FL(使用小的射频刀头在止点区域进行止血)
6. to exposure the corner and media margin of SAP by osteotomy(使用骨凿将磨薄的下关节内缘凿除显露Corner和上关节突内缘)
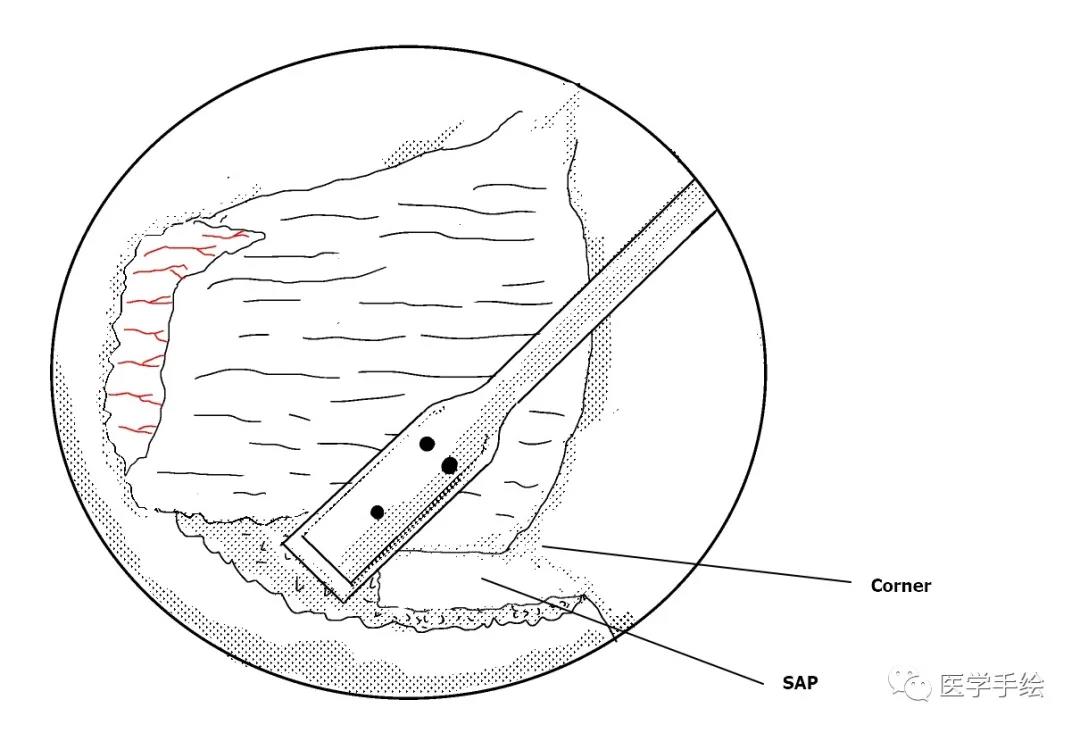
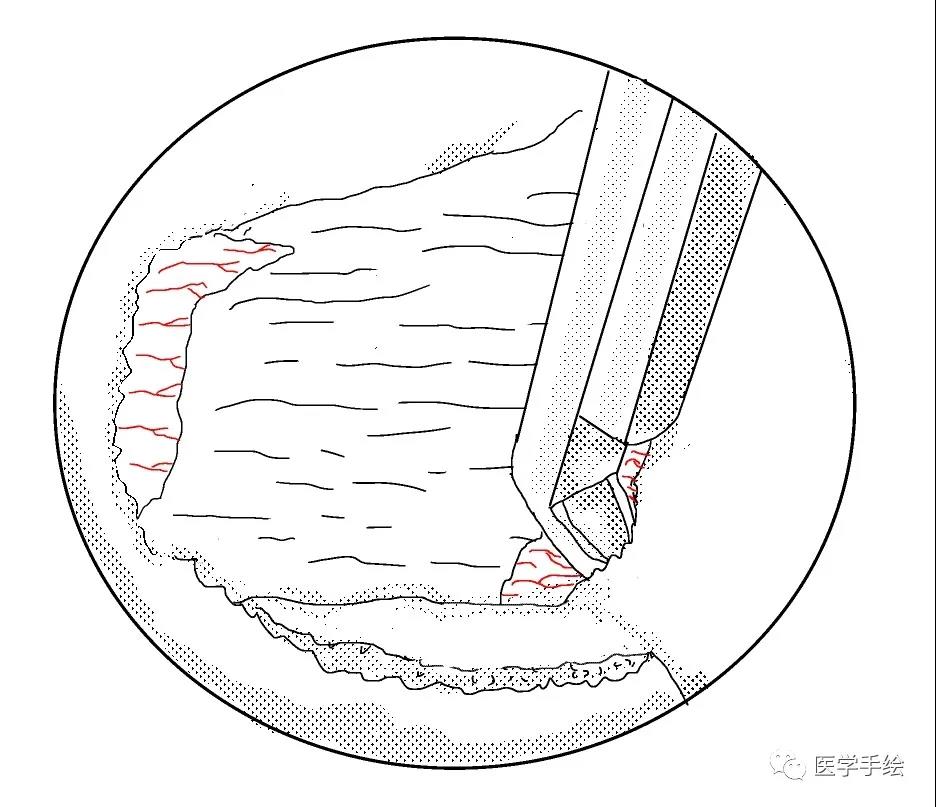
7. the decompression of ipsilateral Corner area by reversed Kerrision Punch(使用反向的椎板咬骨钳减压同侧Corner部位)
8. the lateral edge of decompression is referred to the media margion of pedicle(减压的外界参考椎弓根内壁)
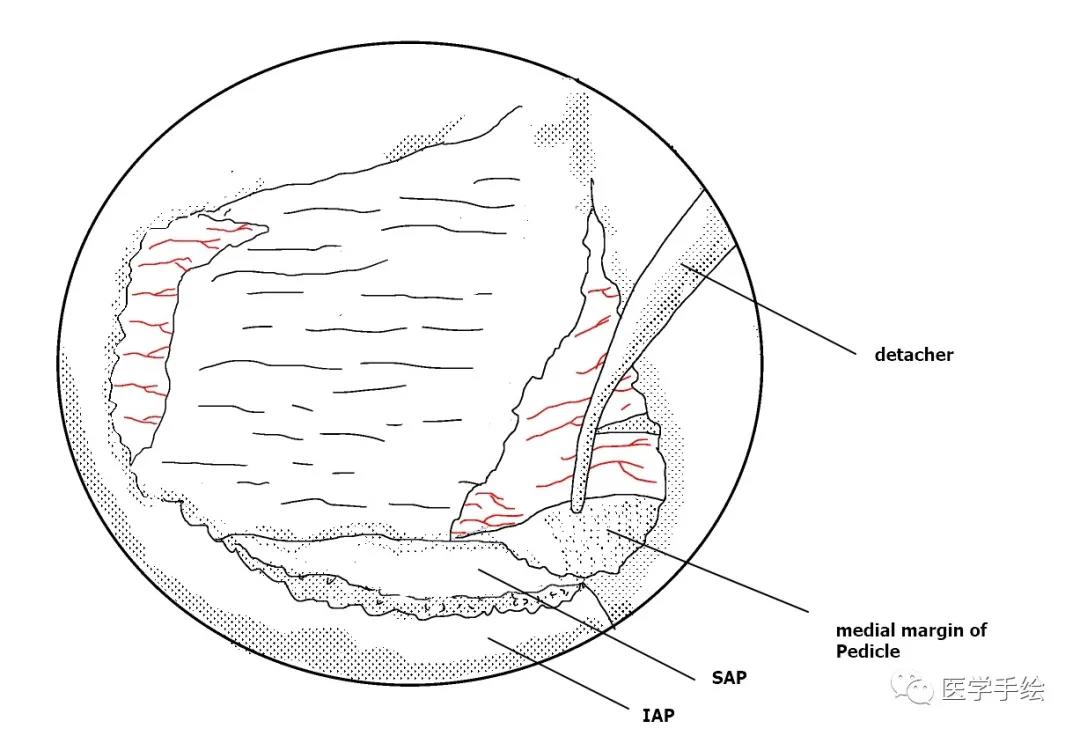
9. to release the lateral margin of FL by removing the media margin of SAP(切除椎弓根内缘同时松解黄韧带外缘)
10. to detach the FL(剥离黄韧带)
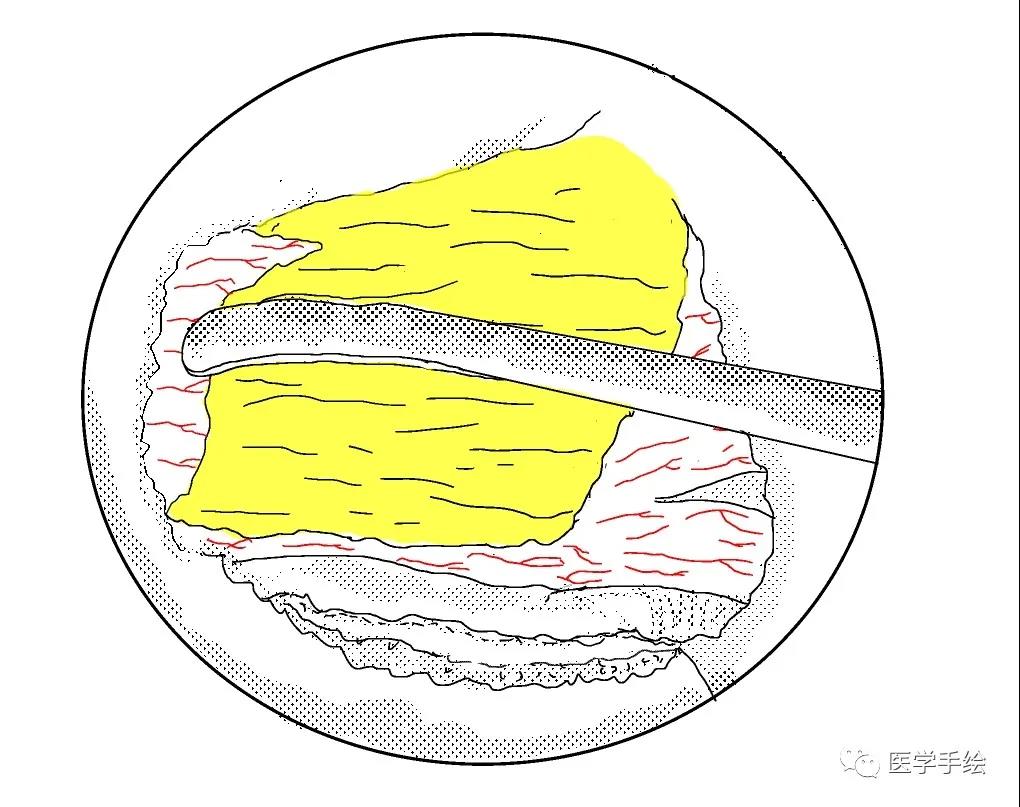
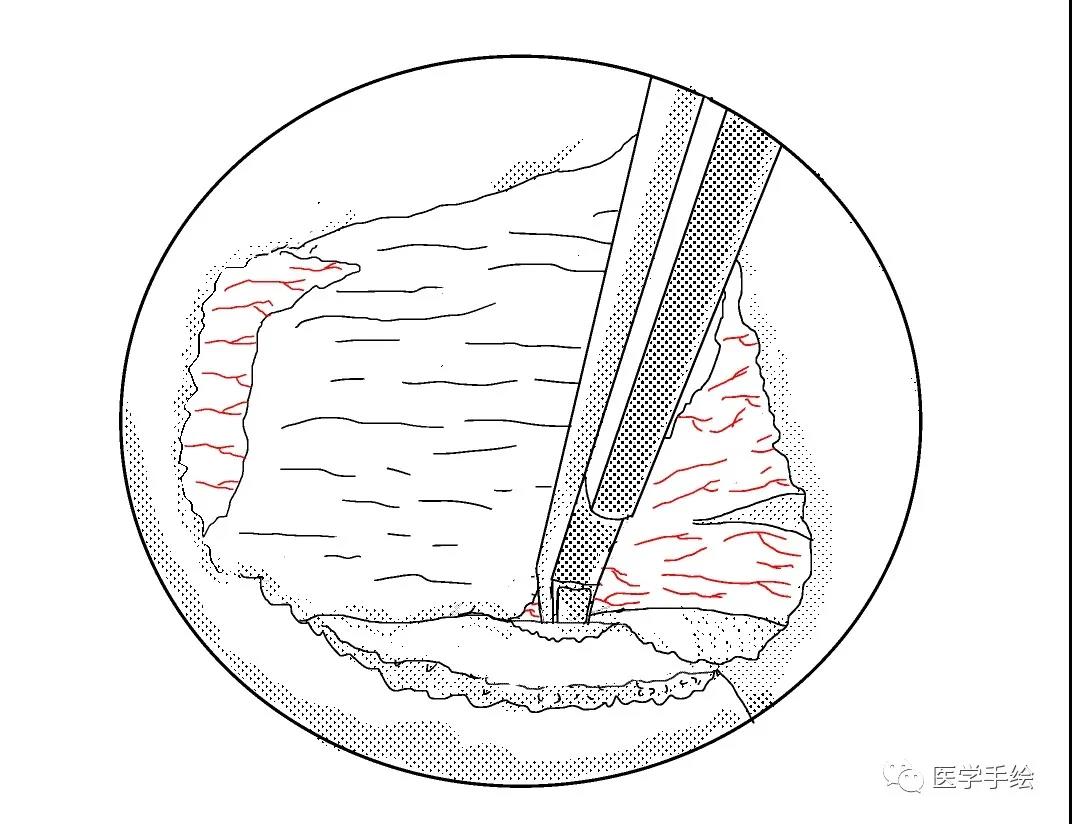
11. to retract the NR(用UBE拉钩牵开神经根)
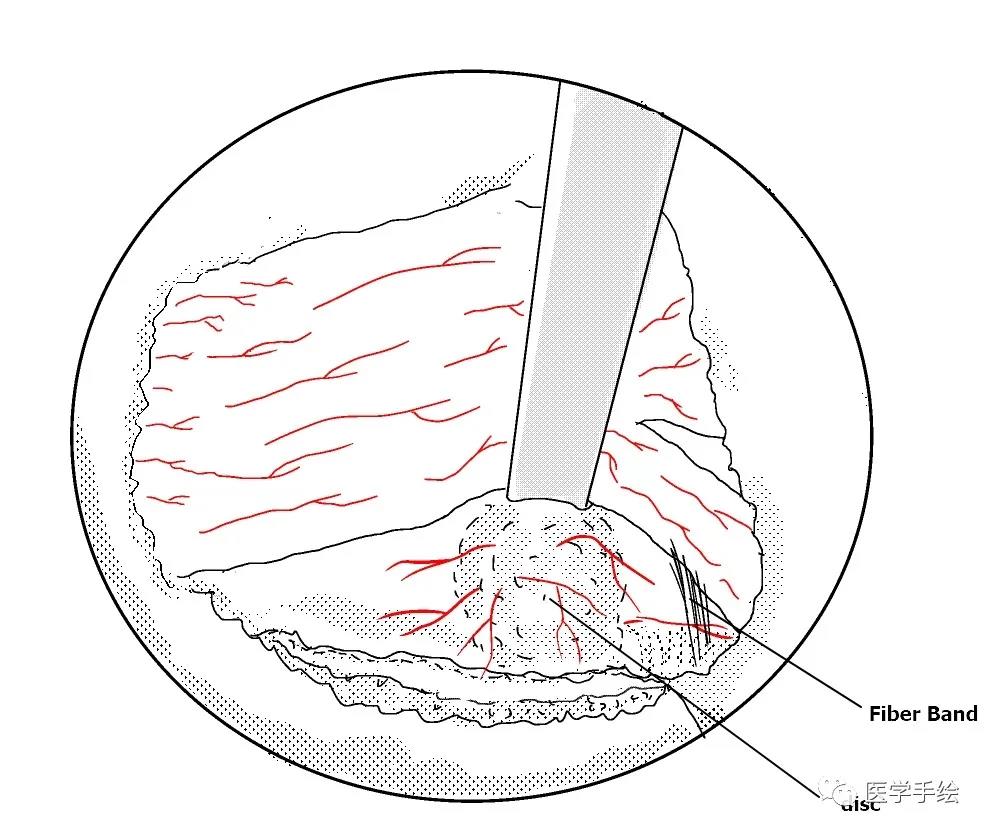
12. bleeding control on the surface of disc and to remove the fiber band around NR(突出间盘表面的预止血和神经根周围束带的切除)
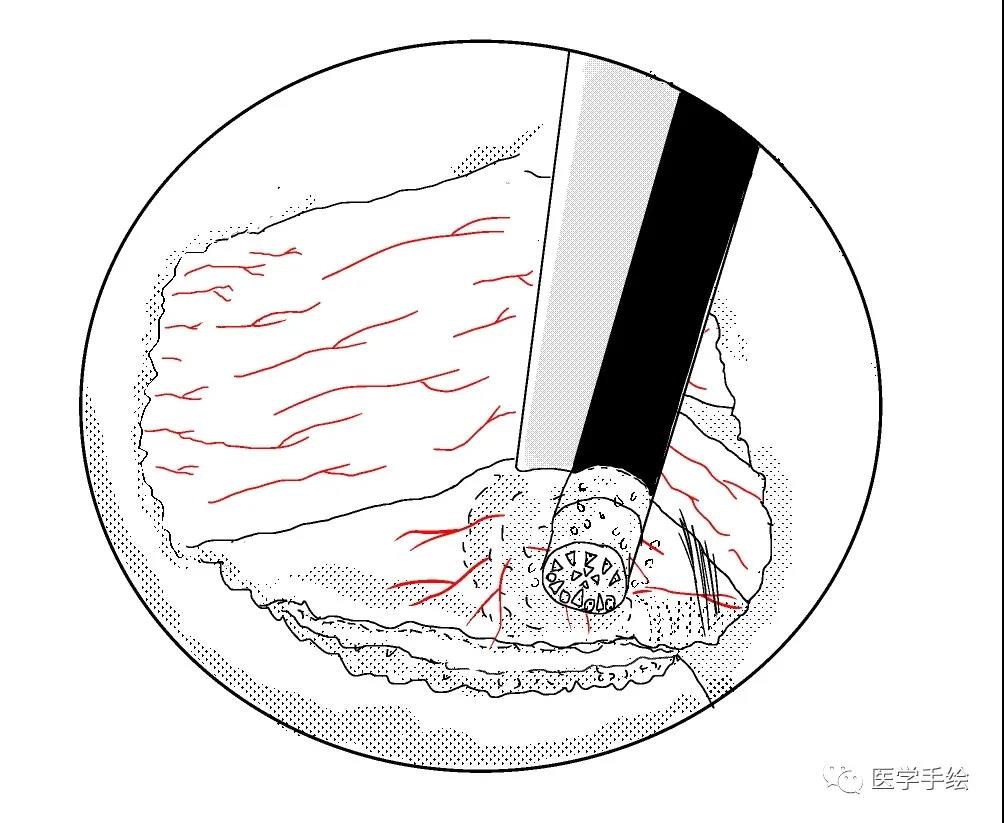
13. to remove the protruding nucleus pulposus by rongeur(使用髓核钳摘除突出的髓核组织)
14. to reduce the size of fissue by coagulation of RF(你可以选择使用等离子电凝皱缩来缩小裂口)
15. or annular suture repair(或者是纤维环缝合修复)
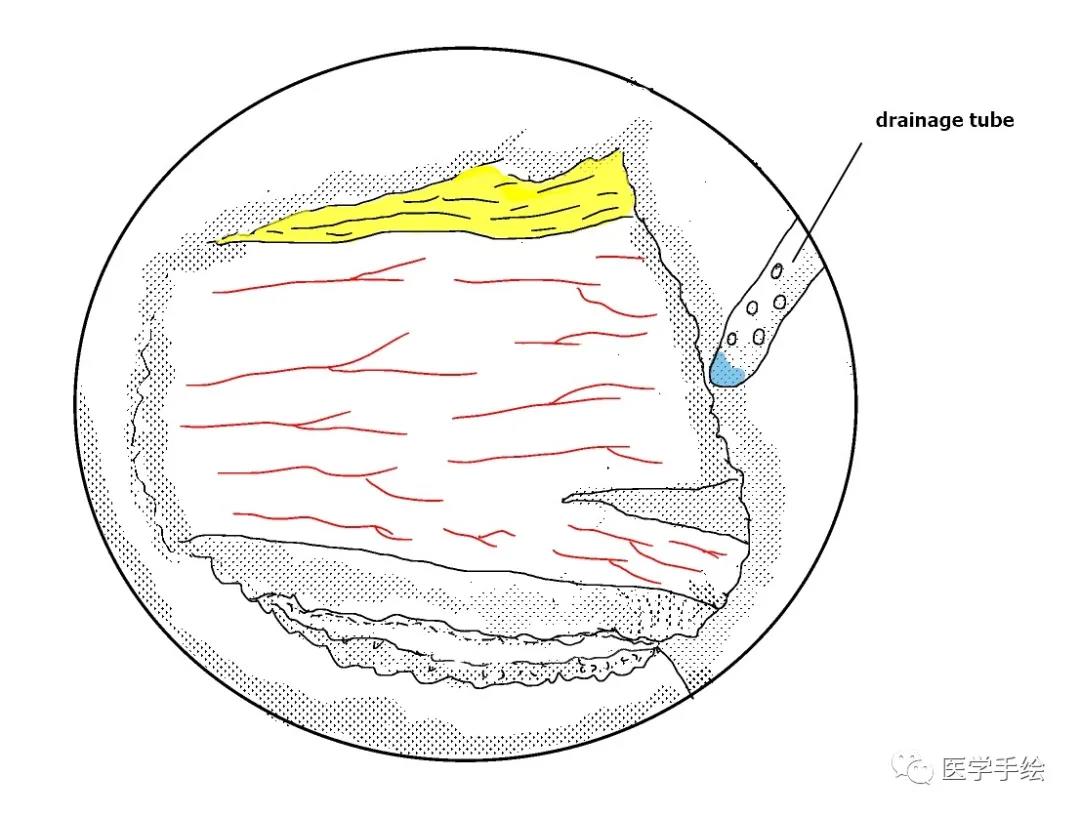
16. It is a good habit to insert a drainage on the surface of lamina at the end of operation(在手术最后放置引流是好习惯,最好放置于椎板表面而不至于干扰神经根)
内容来源于医学手绘